
95% of the gallbladder diseases are cholelithiasis (gallstones.)
About 2% of the US health budget goes towards the management of cholelithiasis and its complications.
10%-20% of the population in the western hemisphere has gallstones.
25-50 tons of the gallstones are carried by more than 20 million Americans.
In the US about 1 million new cases are diagnosed annually, out of these, 2/3 will undergo surgery for the gallstones.
Gallstones are of two main types. 80% are cholesterol stones. Consisting of crystalline cholesterol monohydrate. The remainder are mainly bilirubin calcium salts and are called pigment stones.
The basic reason for the formation of the cholesterol stones is the following:
They only path for the cholesterol removal from the body is via the bile system. Cholesterol is not water soluble. We need to make it water soluble to traverse this path. To solve this, our body forms bile salts and lecithins. These bind with cholesterol and allow the passage through the bile system. These salts and lecithins are like boats on the water to which cholesterol is bound. If the quantity of the cholesterol is more than the binding capacity of these salts, then the unbound cholesterol forms cholesterol monohydrate crystals. These crystals precipitate in solid form. These precipitations irritate the gallbladder layers that in turn release mucus which traps these solid structures in the gallbladder resulting in the stone formation.
In summary, the following four events occur simultaneously for the formation of a gallstone:
1. Amount of cholesterol more than the binding capacity of the bile salts (supersaturation.)
2. Formation of the cholesterol monohydrate crystals.
3. Precipitation and aggregation of these crystals forming solid stone particles.
4. Mucus secretion by the gallbladder's inner surface resulting in the entrapment of these solid particles in the gallbladder.
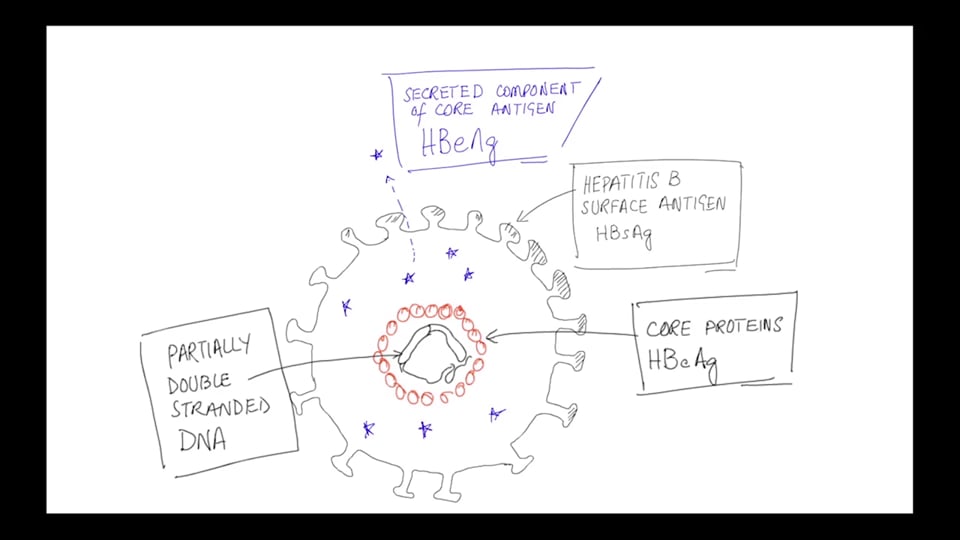
These stones are predominantly composed of bilirubin calcium salts. Their formation is a complex phenomenon. However, it is clear that the presence of unconjugated bilirubin in the bile tree predisposes to the formation of the pigment stones. An example is hemolytic anemia, where the premature RBC breakdown overwhelms the hepatocyte's bilirubin conjugation capacity and the unconjugated bilirubin appears in blood plasma and bile. Infections of the biliary tree can also result in unconjugated bilirubin in the bile.
Also, note that the prevalence of the gallstones is age and gender-related.
Age
Population < 40 has 5% to 6% prevalence of the gallstones.
Population > 80 y has 25% to 30% prevalence of the gallstones.
Gender
Prevalence in white women is twice as high as in men.
Ethnic and geographic
The native American population has a 75% prevalence of cholesterol gallstones. Pigment stones are rare in this group.
Gallstones are more prevalent in western industrialized societies compared to the developing countries.
Robins 8th Edition Page 667
https://www.aafp.org/afp/2004/0115/p299.html
http://eclinpath.com/hematology/anemia/mechanisms-of-anemia/extravascular-hemolysis-new/
Frequently cholelithiasis is asymptomatic. It is usually discovered during a radiographic study or during a surgery, or an autopsy.
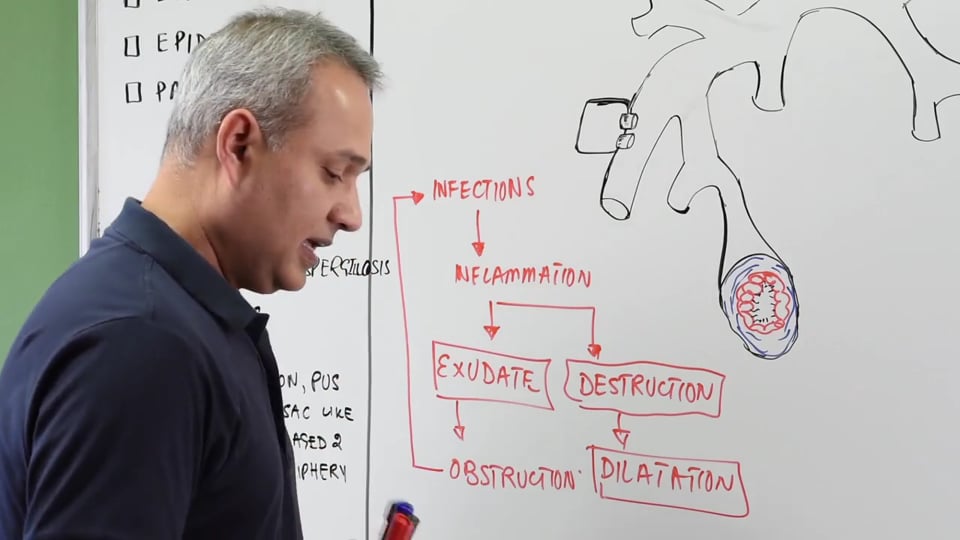
Clinical features of gallstones occur due to the obstruction and inflammation of the gallbladder by a large stone, or the small stones that move down in the biliary tree and get stuck in it, or due to the irritation and inflammation of the biliary tree.
Pain is usually excruciating (severe). It may be constant or colicky. The pain of acute cholecystitis is in the upper right quadrant can be associated with fever, nausea, and a positive Murphy's sign. Biliary or episodic gallbladder pain occurs in 10-25% of the patients. Acute cholecystitis occurs in 20% of these symptomatic patients.
Occasionally gallstone ileus or Bouveret or Mirizzi syndrome occurs as a clinical complication of a gallstone. Bouveret syndrome occurs when the stone obstructs pylorus or duodenum.
Murphy's sign is positive when you palpate the upper right quadrant during inspiration, and the patient's breathing is interrupted or stopped due to the pain.
You can also perform an indirect fist percussion to compare any difference in pain in the right upper quadrant and the left upper quadrant.
Robbins 8th Edition: Page 668
Current Medical Diagnosis and Treatment 2016 - Cholelithiasis chapter.
https://www.youtube.com/watch?v=9L7N89sOSuc
In this video we will learn about:
1. Epidemiology of gallbladder pathologies.
2. Cholesterol stones vs. pigment stones
3. Pathophysiology of cholelithiasis.
4. Prevalence.
5. Clinical presentation and examination findings of acute cholecystitis.
6. Risk factors for acute attacks.
Presented by Dr. Mobeen Syed
Following answers are created by ChatGPT. Occasionally the answer may be harmful, incorrect, false, misleading, incomplete, or limited in knowledge of world. Please contact your doctor for all healthcare decisions. Also, double check the answer provided by the AI below.
In addition to the presenter, following authors may have helped with the content writing, review, or approval:
ACCME Accreditation Statement
The DrBeen Corp is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to
provide continuing medical education for physicians.
AMA Credit Designation Statement
The DrBeen Corp designates this enduring material for a maximum of 0.25 AMA PRA Category 1
Credits™.
Physicians should claim only the credit commensurate with the extent of their participation in the
activity.
In accordance with the disclosure policies of DrBeen Corp and the ACCME (Accreditation Council for
Continuing Medical Education), we are committed to upholding principles of balance, independence,
objectivity, and scientific rigor in all of our Continuing Medical Education (CME) and Continuing
Education (CE) activities. These policies include the careful management and mitigation of any relevant
financial relationships with organizations that are not eligible.
All members of the Activity Planning Committee and presenters have disclosed their relevant financial
relationships. The DrBeen Corp CE Committee has thoroughly reviewed these disclosures and determined
that these relationships are not deemed inappropriate in the context of their respective presentations.
Additionally, they are found to be consistent with the educational objectives and the integrity of the
activity.
| Faculty | Disclosures |
|---|---|
| Dr. Mobeen Syed | Author declares no conflict of interest. |
No credit card information needed.
Ahmed Zaafran, MD
Ahmed Zaafran, MD
Ahmed Zaafran, MD
 0.12 CME
0.12 CME
Dr. Mobeen Syed
Ahmed Zaafran, MD
Ahmed Zaafran, MD
Dr. Mobeen Syed
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.75 CME
0.75 CME
Dr. Mobeen Syed
Ahmed Zaafran, MD
Ahmed Zaafran, MD
Ahmed Zaafran, MD
 0.75 CME
0.75 CME
Tatyana Travkina, MD
Ahmed Zaafran, MD
Ahmed Zaafran, MD

Ahmed Zaafran, MD
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
Dr. Mobeen Syed
 0.17 CME
0.17 CME
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
 1.25 CME
1.25 CME
Dr. Mobeen Syed
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed

Dr. Mobeen Syed

Dr. Mobeen Syed
 0.25 CME
0.25 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.16 CME
0.16 CME
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.20 CME
0.20 CME
Dr. Mobeen Syed
 0.12 CME
0.12 CME
Dr. Mobeen Syed
 0.24 CME
0.24 CME
Dr. Mobeen Syed
 0.19 CME
0.19 CME
Dr. Mobeen Syed
 0.08 CME
0.08 CME
Dr. Mobeen Syed
 0.11 CME
0.11 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.75 CME
0.75 CME
Dr. Mobeen Syed
 0.25 CME
0.25 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.25 CME
0.25 CME
Dr. Mobeen Syed
 0.75 CME
0.75 CME
Dr. Mobeen Syed
 0.09 CME
0.09 CME
Dr. Mobeen Syed
Dr. Mobeen Syed
 0.75 CME
0.75 CME
Dr. Mobeen Syed
Dr. Mobeen Syed
 1.50 CME
1.50 CME
Dr. Mobeen Syed
 1.50 CME
1.50 CME
Dr. Mobeen Syed
 1.50 CME
1.50 CME
Dr. Mobeen Syed
 1.00 CME
1.00 CME
Dr. Mobeen Syed
Dr. Mobeen Syed
 1.50 CME
1.50 CME
Dr. Mobeen Syed
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.75 CME
0.75 CME
Dr. Mobeen Syed
Dr. Mobeen Syed

Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed

Dr. Mobeen Syed
Dr. Mobeen Syed

Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Ahmed Zaafran, MD
Ahmed Zaafran, MD

Ahmed Zaafran, MD
 0.13 CME
0.13 CME
Sameer Islam, MD
 0.50 CME
0.50 CME
Sameer Islam, MD
 0.50 CME
0.50 CME
Sameer Islam, MD
 0.21 CME
0.21 CME
Sameer Islam, MD
 0.75 CME
0.75 CME
Sameer Islam, MD
 1.25 CME
1.25 CME
Sameer Islam, MD
0.20 CME
Dr. Mobeen Syed
 0.25 CME
0.25 CME
Dr. Mobeen Syed
 1.25 CME
1.25 CME
Sameer Islam, MD
 1.00 CME
1.00 CME
Sameer Islam, MD
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Sameer Islam, MD
 0.50 CME
0.50 CME
Sameer Islam, MD
 0.75 CME
0.75 CME
Bilal Hameed, MD
 0.15 CME
0.15 CME
Sameer Islam, MD
Ahmed Zaafran, MD
Ahmed Zaafran, MD
Adam Jones MD
 1.75 CME
1.75 CME
Amr Madkour, MD
 2.00 CME
2.00 CME
Mir Alikhan, MD
Ahmed Zaafran, MD
Ahmed Zaafran, MD
Mir Alikhan, MD
Mir Alikhan, MD
Mir Alikhan, MD
Mir Alikhan, MD
Ahmed Zaafran, MD
Ahmed Zaafran, MD
Ahmed Zaafran, MD
 0.75 CME
0.75 CME
Dr. Mobeen Syed
Ana Crawford M.D., M.Sc.
Ana Crawford M.D., M.Sc.
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Ana Crawford M.D., M.Sc.
Ana Crawford M.D., M.Sc.
Ana Crawford M.D., M.Sc.
Ahmed Zaafran, MD
Ahmed Zaafran, MD
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
 0.21 CME
0.21 CME
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
 0.25 CME
0.25 CME
Dr. Mobeen Syed
 1.00 CME
1.00 CME
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
 1.25 CME
1.25 CME
Zaina Al-Mohtaseb, MD
 1.00 CME
1.00 CME
Zaina Al-Mohtaseb, MD
Tabraiz Mohammed, MD
Tabraiz Mohammed, MD
Tabraiz Mohammed, MD
Ahmed Zaafran, MD
 0.25 CME
0.25 CME
Hatem Abou-Sayed, MD
Ahmed Zaafran, MD
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
 0.25 CME
0.25 CME
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
 0.23 CME
0.23 CME
Dr. Mobeen Syed
 0.25 CME
0.25 CME
Dr. Mobeen Syed
 1.00 CME
1.00 CME
Dr. Mobeen Syed
 0.25 CME
0.25 CME
Dr. Mobeen Syed
 0.25 CME
0.25 CME
Dr. Mobeen Syed
 0.25 CME
0.25 CME
Dr. Mobeen Syed
 1.00 CME
1.00 CME
Luis A Verduzco M.D.
 0.25 CME
0.25 CME
Dr. Mobeen Syed
 0.75 CME
0.75 CME
Dr. Mobeen Syed
Tim Wang, MD
Dr. Mobeen Syed
Dr. Mobeen Syed
Tim Wang, MD

Tim Wang, MD
Ahmed Zaafran, MD
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 1.00 CME
1.00 CME
Dr. Mobeen Syed
 0.22 CME
0.22 CME
Dr. Mobeen Syed
 0.25 CME
0.25 CME
Dr. Mobeen Syed
Dr. Mobeen Syed
 0.25 CME
0.25 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.23 CME
0.23 CME
Dr. Mobeen Syed
 0.75 CME
0.75 CME
Dr. Mobeen Syed
Ahmed Zaafran, MD
 0.25 CME
0.25 CME
Ana Crawford M.D., M.Sc.

Ana Crawford M.D., M.Sc.
 0.75 CME
0.75 CME
Dr. Mobeen Syed
 0.25 CME
0.25 CME
Dr. Mobeen Syed
 0.25 CME
0.25 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.25 CME
0.25 CME
Dr. Mobeen Syed
 0.75 CME
0.75 CME
Dr. Mobeen Syed
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 0.22 CME
0.22 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed
 1.00 CME
1.00 CME
Dr. Mobeen Syed
Dr. Mobeen Syed
 0.75 CME
0.75 CME
Dr. Mobeen Syed
 1.00 CME
1.00 CME
Dr. Mobeen Syed
 1.25 CME
1.25 CME
Dr. Mobeen Syed
 0.23 CME
0.23 CME
Dr. Mobeen Syed
 1.25 CME
1.25 CME
Dr. Mobeen Syed

Dr. Mobeen Syed
0.75 CME
Dr. Mobeen Syed
 0.50 CME
0.50 CME
Dr. Mobeen Syed

Dr. Mobeen Syed
Dr. Mobeen Syed
 0.75 CME
0.75 CME
Dr. Mobeen Syed

Dr. Mobeen Syed
Dr. Mobeen Syed

Hatem Abou-Sayed, MD
Tammy Wang, MD
Dr. C. Merry
All information contained in and produced by DrBeen corp is provided for educational purposes only. This information should not be used for the diagnosis or treatment of any health problem or disease.
THIS INFORMATION IS NOT INTENDED TO REPLACE CLINICAL JUDGMENT OR GUIDE INDIVIDUAL PATIENT CARE IN ANY MANNER.
Click here for notice and disclaimer.
Write A New Comment
2 Comments
jay9635.presswala@*.com
Oct 16 2020, 6:59 pm
Hello sir i m here for diagrammatic representation and more dynamic understanding of this disease but here i am getting podcast of this disease...... is this correct way for study???
Also sir i am disappointed by acute abdomen series the tutor in volume 1 only explaimed 1 sign and then tutor in volume 2 in acute appendicitis told that we have already discussed all the signs in vol.1
Now sir u tell me whom to beileve coz signs arent discussed in any lecture
Also sir i m quite disappointed with dr been subrcription i thought it would be more diagrammatic and clinical feature but i was wrong
But i also appreciate all your efforts in ecg series i have watched it thoroughly and i am quite satisfied by that series
I hope you will improve some of the content
watstewart@*.com
Aug 14 2019, 5:22 am
I find it interesting the issues that people have post choleycystectomy. It seems as though it brings on a new series of chronic issues. For example, increasing serum bile acid levels, the changes in pH in the intestines, the different composition of bile that freely flows into the intestines vs the composition of gallbladder bile that is concentrated. The changes in the signalling system with the FGF-19. The increased risk for colon cancer. Thanks for the lecture Dr. Mobeen. It's a pleasure.